Here’s an October 2021 update on my quest to reduce arterial stiffness. For the original story and context, see previous post here.
After a year of >15 000 steps/day, continued adherence to improved nutrition, and a modified training approach, I saw another nice reduction in carotid-femoral pulse wave velocity (cf-PWV) along with an increase in RMSSD (see figure below).


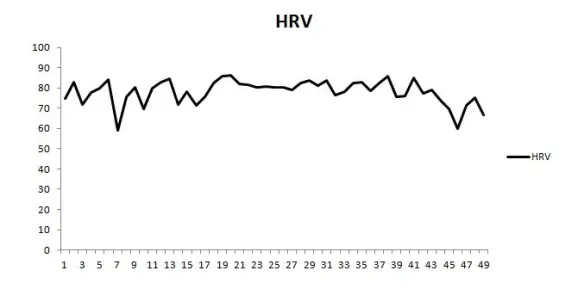
RMSSD values (post-waking, standing position) from this October were the highest I’ve recorded to date. It seems that the more I try to reduce cf-PWV and improve my cardiovascular health, the more my HRV increases, despite no change in RHR. This strengthens my view that HRV can be an effective behavior-modification tool for health.

An important training modification that I implemented this October was changing my 10-min post-lift steady state air bike ride to intervals. The protocol is simply to pedal hard (though sub-maximally) for the first 10 s of every min for 10 min (excluding the first minute). Over ~4 weeks my “sprint” intensity naturally increased from ~450-500 to ~500-550 watts and recovery intensity from ~150 to ~180 watts. I’m pretty confident that this change accounts for the further increase in RMSSD. I performed a very similar protocol back in 2014 (post-lift intervals, 2014 figure re-posted below) for 2 weeks and saw an immediate increase and stabilization in my RMSSD values (middle of trend, LnRMSSDx20), which reverted to “normal” after cessation. My October 2021 PWV assessment occurred 2 weeks after starting this protocol, so it’s hard to say how much this may have had an effect.
Post-RT interval training may be a more time-efficient method to counteract the intense RT-induced arterial stiffening. Studies have shown that 30 min steady state, or 10 min of intervals on a bike attenuate post-RT increases in cf-PWV. Only 10 min of steady state riding attenuates RT-induced endothelial dysfunction (which is what originally inspired me to include this after my lifts). In terms of practicality, most lifters will unlikely perform 30 min of aerobic work post-RT. Ten min may be an easier sell. The intervals I’ve been experimenting with may be intense enough to provoke the desired effects, though short and submaximal enough for long-term use. Spearheaded by my incredibly intelligent and competent GA, Joe Vondrasek, we plan to investigate this further next year. We need to determine how such a protocol impacts both cardiovascular health markers and RT adaptations (i.e., day-to-day recovery, interference effect, etc).
I’m happy with the progress I’ve made thus far in reducing arterial stiffness (8.6 to 7.2 m/s). For context, below are norms for cf-PWV from this study. My values are now much closer to norms for my age group. Moving forward, my goal is to resume heavier powerlifting training while maintaining step-count, post-lift interval training, and aerobic work on non-lifting days to see if I can keep PWV under control while building my strength back up to respectable levels.

