I posted some data a couple of months ago comparing my HRV to my tap test results to see if there was any correlation between the two. You can see that post here if you missed it. It was around that time that I also started using a Reaction Test app. Today I’ll be posting and reviewing my Reaction Test data with my HRV data to see what it might reveal. At the end of the post I’ll provide some brief updates on what’s been happening since I started working in the Human Performance Lab here at Auburn (Montgomery).
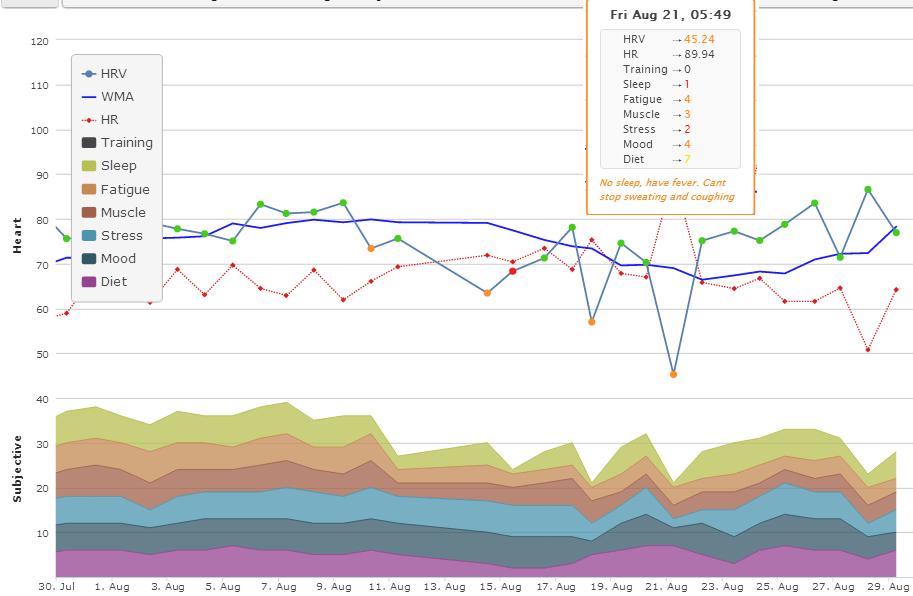
HRV: I continue to use ithlete as my main HRV metric. Daily measurements are performed each morning after waking and bladder emptying. All measurements are performed in the standing position with paced breathing. The HRV value provided by ithlete is Ln RMSSD x 20; a time domain measure of parasympathetic tone.
Reaction Test: The reaction test is performed after my HRV test and my Tap test (I’m still doing these but will not include them today). All reaction tests were performed using right index finger. The app functions as follows;
- initiate app
- Tap target area to start the test
- React to stimuli (color change) as fast as possible by tapping the screen
- Repeat for a total of 5 reactions (variable time intervals between)

I used excel to calculate daily average with the reaction test data (plotted on the charts below).
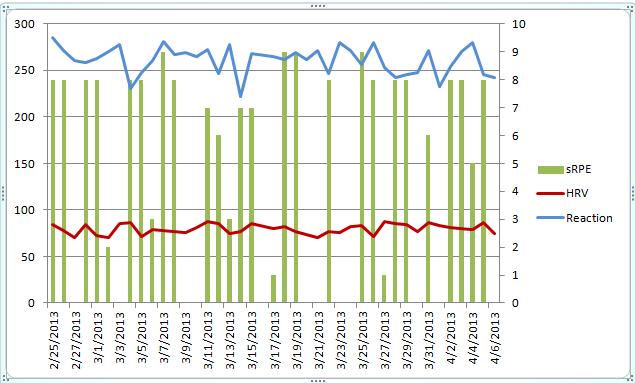
Keep in mind that for a correlation between high HRV and good Reaction Test, we want to see an inverse relationship in the trends. We’re looking for a fast Reaction time (trending down) with a higher HRV score (trending up).
Chart 1 – HRV, Reaction Test Average and Session RPE (secondary axis)

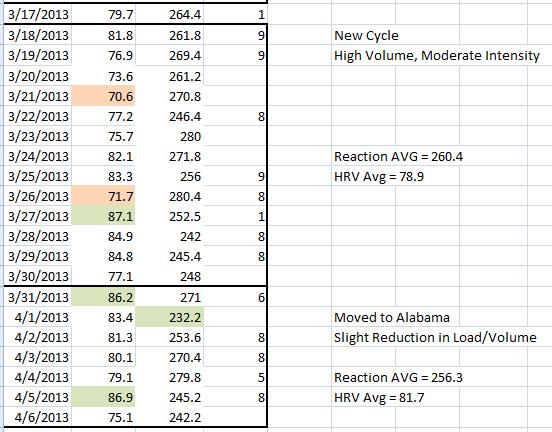
For more clarity I’ve also included excel screen shots of the raw data. I’ve sectioned off 4 different areas and noted the goal/purpose of that particular time of training. It works out so that there is a High Intensity section, a Deload section, a High Volume Section, and a Semi-Deload section. The “Semi-Deload” period occurs over the past week that I’ve moved to Alabama. I figured it would be wise to scale intensity and volume back very slightly while I settle in to a new place and new work environment. To give an example, I essentially removed a main working set and stuck with familiar weights. Assistance work was relatively unchanged.


* I must have forgotten to perform a reaction test or forgot to save it on 03/16 which was a Saturday and therefore it is not included.
I’ve highlighted any score that was +/- 10% from the total average. So for exampme; if HRV was 10% higher than the average of all HRV scores, I would shade that day green. Likewise for Reaction Test. Red shading denotes 10% or greater reduction.
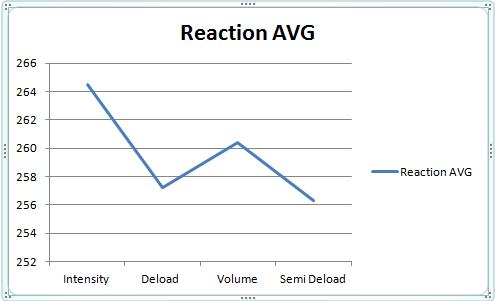
After examining the acute relationship between Reaction Test and HRV I decided to examine the averages for each training block. I’ve shifted my focus lately a little bit more on weekly trend changes vs. daily trend changes. As you can see in the charts below, there is a very strong relationship between HRV AVG and Reaction Test AVG during each training section.

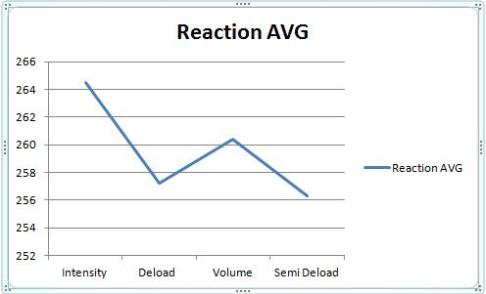
– Intensity Section – This section was the last 2 weeks of my 9 week training cycle that I performed after the Christmas break (discussed here). Volume was low but intensity was Maximal. HRV is at it’s lowest average while Reaction Test is at its highest (slowest reaction time) average.
– Deload – During the deload week HRV average rebounds to peak levels while reaction time improves to near peak levels.
– High Volume – This marks the start of a new training cycle. HRV drops quite a bit and Reaction Time average increases (slower reaction).
– Semi-Deload – HRV returns to near peak values while Reaction Test peaks (quickest reaction time average).
From this data set, intensity appeared to have the biggest effect on Reaction Test average and HRV average. High volume work with moderate intensity also had a significant impact on these averages. It should be kept in mind that the Intensity period followed several weeks of training and therefore some fatigue had already been accumulated. I didn’t start using the reaction test until late February. HRV and Reaction averages improve over periods of reduced training load.
Given that I was able to hit some PR’s in the gym during the Intensity section (under high fatigue), I’m inclined to say at this point, based on this data set, that these tests are not necessarily indicators of performance potential (strength), but rather markers of fatigue. In the future I would like to see how these tests match up with “finer” motor skills in other athletes.
Quick Updates
I made it safely to Montgomery, AL after a nice visit with some family at my folks place in Cincinnati over Easter. Total travel time was about 17.5 hours. We wasted no time in getting to work in the lab. We’ve got 3 projects going on right now (the first two being more health related as opposed to sports/performance).
- I’m helping Dr. Esco complete a study comparing post-exercise HRV recovery after two different modes of exercise (cycling vs. treadmill at same intensity/duration).
- We are starting a new study comparing post-exercise HRV in middle aged men after 3 modes or resistance training; Eccentric only; Concentric Only; Traditional Resistance Training
- We have put the wheels in motion for a cross-validation study comparing ithlete to EKG. We did some pilot work with about 6 subjects so far and have IRB Forms and Consent Forms about ready for submission. We’ll measure ithlete and EKG simultaneously in about 20 males and 20 females then run the data. This is a very important study to me. In order to improve what we know about HRV and performance, we need more data. Using EKG’s in the field is not practical. What we need to start seeing is data from athletes that are performing measurements at home when they wake up. The device needs to be extremely easy to use and the data needs to be immediately available to the coach. At this time, smart phone app’s are the best way to do this. There are plenty of limitations with this but at the end of the day, if we’re going to apply this stuff in a team setting we need easy to use, affordable tools.
- This last project doesn’t exist yet. But I’m hoping to collect data on either the men’s tennis team or the women’s soccer team. I’ll provide more info on this if and when it starts to take shape.
Let me be clear right from the start in saying that Dr. Esco is running the show here. I’ve learned a ton from him already about the research process and anything that I accomplish over the next little while will be because of him.
Lastly, I attended my first Roller Derby which was quite the experience.