Highlights from our latest study in JSCR. Full-text available here.
We aimed to determine how 10 min of post-resistance exercise cycling affects aortic stiffness responses and next day recovery markers in well-trained men.
– A 10-min bout of air bike cycling was ineffective at countering acute RE-induced increases in cfPWV (aortic stiffness), likely because of the rapid and unanticipated cfPWV return to baseline by Post-RE 15min in both conditions (intervention & control).
– Accelerated post-RE cfPWV normalization may be an adaptation to habitual RE, as acute RE-induced aortic stiffness typically persists for >60 min in less experienced lifters.
– Thus, targeting the attenuation of acute post-RE increases in cfPWV is likely unnecessary, but whether the intervention exerts chronic effects, such as limiting long-term RT-induced increases in resting cfPWV, remains TBD.
– Despite no effect of the intervention on cfPWV at the group level, it altered changes at the individual level, such that those with a lower relative cycling power output at the target HR exhibited greater reductions in cfPWV.
– This may indicate that lifters with lower aerobic fitness may derive greater AE-induced destiffening effects after acute RE. – Finally, the AE intervention neither enhanced nor impaired recovery indicators (HRV, subjective, barbell velocity), alleviating concerns about short-term AE interfering with next-day recovery status or performance.
We aimed to quantify associations between resting heart rate variability (HRV) and ambulatory blood pressure (BP) characteristics in young adults. Thirty-two apparently healthy young adults (50% male) were included in the study. Short-term HRV was obtained via electrocardiography in the laboratory following an overnight fast to determine the mean RR interval, standard deviation of normal RR intervals (SDNN), and root-mean square of successive differences (RMSSD). Participants left the laboratory wearing an ambulatory BP monitor for 24 h to determine awake, asleep, and overall systolic and diastolic BP, and asleep BP dipping ratios. In males, higher SDNN and RMSSD were associated with lower asleep systolic and diastolic BP, and greater systolic BP dipping, with SDNN also associated with diastolic BP dipping (Ps <0.05). In females, higher mean RR, RMSSD, and SDNN were associated with lower awake diastolic BP, and RMSSD with lower overall diastolic BP (Ps <0.05). Our findings indicate potential sex differences in how cardiac-autonomic function associates with BP regulation throughout the day. In males, HRV showed stronger associations with nocturnal BP characteristics, whereas in females, HRV associations were more pronounced with daytime BP.
New study: “Effects of Position and Injury Status on Associations Between Preseason Workload and Heart-Rate Variability Profiles in American College Football Players”
Main findings:
The effect of very high preseason training loads on HRV in college football players varies by position group.
Skill group players who consistently performed the highest total workloads had the most stable HRV, which typically reflects high/increasing fitness.
Conversely, mid-skill group players who performed the highest total workloads had the least stable HRV (often reflects fatigue), along with greater daily variation in high intensity outputs.
Thus, skill players tolerated high loads with stable HRV while mid-skill players better maintained high intensity movement and stable HRV at more moderate workloads.
HRV tended to be lower in those who were playing hurt (“go as can” status), and we suspect that the association between HRV and injury is bidirectional (low HRV precedes injury, injury causes reduced HRV).
Here’s a new study from our lab entitled “Self-recorded heart rate variability profiles are associated with health and lifestyle markers in young adults”. The full text can be accessed for free through this link: https://rdcu.be/cUd9T. A practical summary is provided below.
We’ve been tracking ANS status in athletes via daily ultra-short HRV for nearly 10 years now. In general, we (and others) have found that higher and more stable values are often observed in athletes who are more aerobically fit and who are adapting well to training. Contrastingly, lower and less stable values are commonly observed when athletes are stressed, fatigued from training, and not adapting favorably.
There is also a sizable body of research showing that isolated HRV derived from clinical and laboratory assessment is associated with a variety of health and lifestyle markers in general and clinical populations. Healthier individuals tend to have higher vagal-mediated HRV, are less likely to develop chronic diseases, and often live longer. There is also research showing that less stable HR parameters (i.e., greater day-to-day fluctuation) are independently associated with an increased risk of cardiovascular events in older adults. Importantly, HRV is modifiable. With lifestyle improvement, one can make their HRV higher and more stable. Here’s a case example showing substantial improvements in HRV and other healthy markers with improvements in various lifestyle factors: https://hrvtraining.com/2021/08/10/increasing-hrv-and-cardiovascular-health-10-year-case-study/.
Thus, similar to how we track HRV in athletes to guide training and monitor adaptations, we hypothesize that regular folks can track their HRV to guide lifestyle behaviors towards those that increase cardiac-parasympathetic function, thereby supporting health and longevity. However, no previous investigations have examined the association between self-recorded HRV and health/lifestyle metrics in young adults using accessible HRV tools and ultra-short (60-s) daily recordings. Therefore, that’s what we set out to do.
We had subjects perform 60-s post-waking HRV recordings in the supine and standing position with a cost-free smartphone application and Bluetooth chest strap for 7 days. They also wore an Actigraph on their wrist to measure activity levels and sleep profiles. Following the observation period, we obtained a variety of cardiovascular, metabolic, and psychoemotional health markers in the laboratory.
As anticipated, higher and/or more stable HRV parameters were generally associated with more favorable cardiovascular (higher VO2max, lower systolic and diastolic blood pressure, and lower aortic stiffness), metabolic (lower body fat percentage, fasting glucose, and LDL-C), and psychoemotional (lower perceived stress) health markers. Some variation between sexes and recording positions were noted. Additionally, most, but not all, associations weakened after adjusting for VO2max, supporting previous work indicating that increasing fitness is one of the most effective ways to increase HRV and derive health benefits associated with increased parasympathetic (and reduced sympathetic) modulation. For more details and conclusions, see the full text here: https://rdcu.be/cUd9T
If success leaves clues, then there was something to learn from what Dan Howells & staff did to prepare GB 7s for the 2016 Olympics where they advanced to the gold medal final with an undefeated record.
After sorting through the data (HRV, wellness, training load) and having several video and email conversations with Dan, we decided to share the story of their Olympic expedition.
Prior to analyzing the data or obtaining specific details from Dan, I anticipated substantial decrements in status markers in response to a full day in transit (travel fatigue/jet lag, etc.), pre-tournament (arousal/anxiety), & throughout the tournament (match fatigue, sleep loss).
However, data showed minimal effects of travel (decrements mostly in non-starters), no evidence of pre-competitive anxiety (values improved pre-match), & intra-tournament decrements (small in magnitude) comparable to a previous domestic tournament.
Essentially, the data suggest that the team travelled across multiple time zones, adjusted to a foreign environment, and competed successfully on the worlds biggest stage with hardly any indication of stress or fatigue. Incredible!
Although we can’t say for sure that the strategies employed by staff can explain the findings (no control group, unfortunately), we felt that the details were worth sharing.
The paper discusses various proactive and reactive interventions that were used to support training adaptation, manage travel and competition related stress/fatigue, and aid recovery in players.
I’m very grateful to Dan and staff for the collaboration and for being open with these details. There is tremendous vulnerability in giving everyone access to how you do things. Thank you, Dan. You shared tremendous insights that many coaches and players can benefit from.
As part of my PhD work at Alabama, we tracked HRV in football players from day 1 of preseason training through to the national championship. A practical summary of some key findings follow the full-text link below.
Fluctuations in HRV are expected throughout a season. However, chronically suppressed values are cause for concern. Sustained parasympathetic hypoactivity is associated with various pathological conditions and is a hallmark of stress and impaired recovery in athletes.
We learned from spring camp that day-to-day HRV recovery was delayed in linemen vs. the smaller and more aerobically fit skill players. Thus, we anticipated that linemen would be more susceptible to attenuated HRV throughout the season.
HRV started to decline by week 6 of the competitive period for linemen. A couple notable events occurred here: 1) the first of 5 consecutive SEC match-ups vs Top 25 nationally-ranked opponents and 2) the week of mid-term exams for many players.
Although significant group-level reductions for linemen weren’t observed until later, key players showed descending HRV by mid-season, in the absence of changes in PlayerLoad. Suppressed HRV preceded illness and injury in 2 starters. Temporary rest restored HRV.
Group-level reductions occurred during an intensive camp-style preparation period for the college football playoffs following the SEC championship. Most players took a hit to their HRV, but linemen were hit the hardest. Note magnitudes of the effect sizes in the table below.
HRV remain suppressed for linemen through prep weeks for the national semi-final and the national championship. Smaller decrements (non-significant) were observed for skill players. In addition to accumulating physical stress, psycho-emotional factors (pre-competitive anxiety, pressure to perform, media attention, etc) likely contributed.
Although we emphasize the toll of a season on linemen, some skill players also showed suppressed values. The table below shows the rate of change in HRV for all players. 25% of skill and 63% of linemen showed sig. descending HRV patterns throughout the season.
Linemen experience hypertension, arterial stiffening, and pathologic LV hypertrophy following 1 or more seasons. These maladaptations are possibly preceded by ANS imbalance. We hypothesize that larger players showing the worst HRV profiles suffer the greatest decrement in cardiovascular health markers.
If so, intervening when a decreasing HRV pattern is observed may not only be relevant to performance (limiting fatigue, injury-, and infection-risk), it may also help mitigate the cardiovascular toll of playing football at such a high level. Seeking funding to explore this in the future.
The findings highlight potential deficiencies in or greater taxation to the coping capacity of linemen vs. smaller players. Factors hypothesized to contribute to more prevalent ANS imbalance in linemen and potential implications for health and performance are summarized below.
Linemen need careful attention and monitoring. We need strategies to prevent ANS imbalance from occurring (load management, aerobic capacity, treatment of health conditions like sleep apnea, etc) and we need restorative methods to implement if it occurs.
Tracking HRV with a mobile app was inexpensive and easy. Time-demand from players was ~3 min/week while waiting to get taped. Though sub-optimal relative to post-waking measures, this approach enabled timely detection of descending patterns, which may be useful for guiding interventions relevant to player health and wellbeing.
Though a better understanding of the health and performance ramifications of suppressed HRV in football players is needed, a descending pattern may serve as an easily identifiable red flag requiring attention from performance and medical staff.
When first getting started with tracking HRV in athletes, the inter-individual variation in trend characteristics can be confusing. Some athletes will display very high values and others will show lower values. Likewise, some will show quite stable values while others display substantial day-to-day variation. Naturally, the following question arises: why do some athletes have higher and more stable values than others?
Collegiate swim rosters typically include a mixed roster of athletes (males and females with a broad range of experience and skill). In this investigation we compared HRV trend characteristics between the national-level (including 6 Olympians) and conference-level sprint-swimmers throughout 4 weeks of standardized preparatory training. We also obtained details of individual training history.
The main findings were that national-level swimmers had higher and more stable HRV (higher mean LnRMSSD, lower LnRMSSD coefficient of variation) than their conference-level teammates. Differences in trend characteristics were attributable to a greater history of training and competing among the national-level swimmers (i.e., greater training age).
Whether these findings can be explained by greater aerobic fitness (we don’t think so), greater familiarity with training (possibly), or chronic physiological adaptations (possibly) among the higher-level swimmers is unclear.
The findings may be of some practical use for coaches when interpreted with previous work (see links below). For example, preliminary expectations with HRV monitoring should be that higher-level swimmers will display higher and more stable values throughout training and vice-versa for lower-level athletes. This may be interpreted to mean that the higher-level athletes could tolerate greater loads or that the lower-level athletes may need reduced loads. However, it is unclear if these training modifications would offer any performance/adaptation advantage. In addition, a higher-level athlete showing lower and less-stable values may be cause for concern (fatigue, stress, detraining, etc. depending on context). Whereas a lower-level athlete displaying higher and more stable values is likely adapting well to the training.
We’ve previously assessed how overload and tapering impact HRV in sprint-swimmers here.
We’ve previously assessed associations between subjective indicators of recovery and daily HRV in sprint-swimmers here.
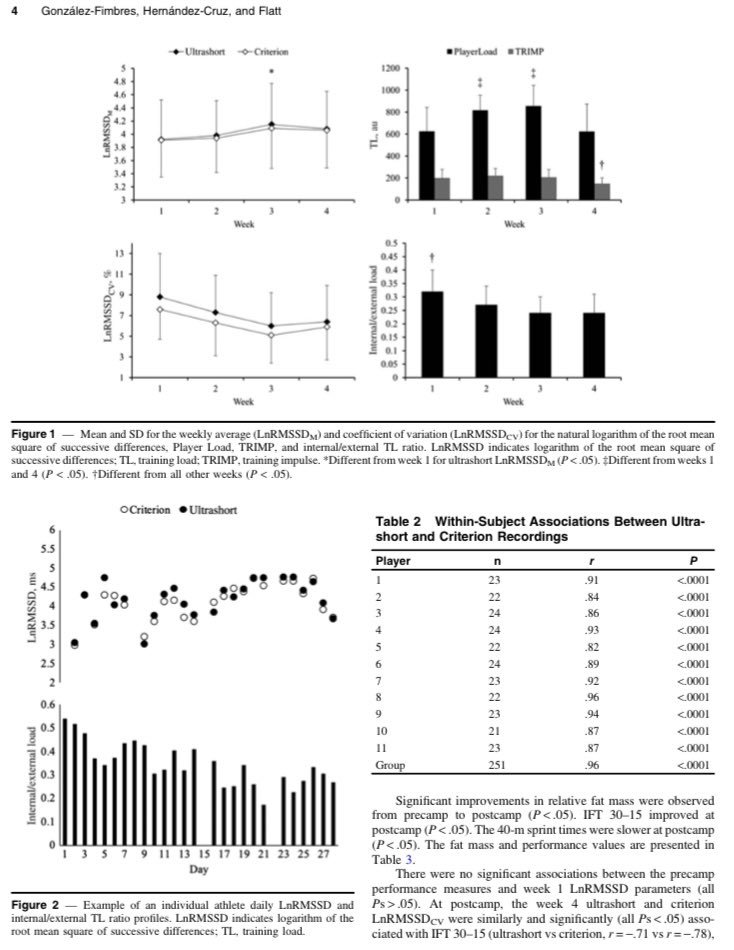
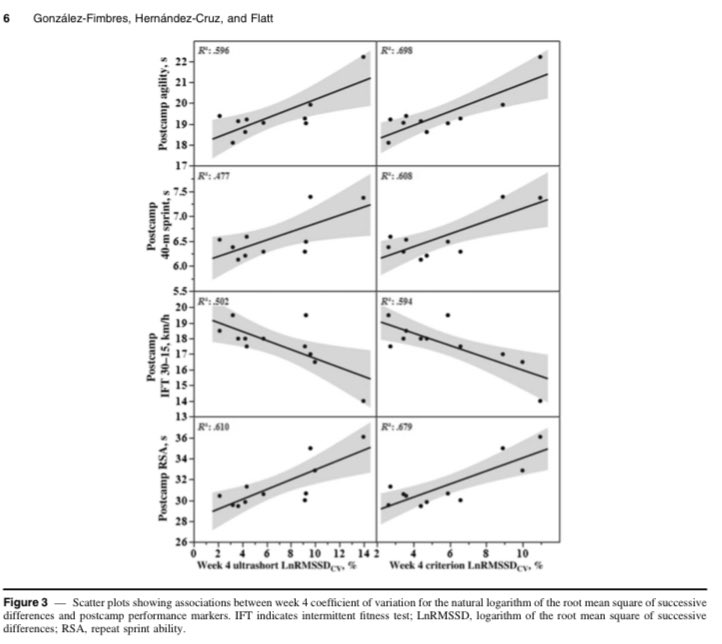
Here’s our latest study comparing 1 min vs 5 min HRV throughout a 4-week camp in international-level girls field hockey players. Values were highly correlated, showed similar responses to load, & similar associations with fitness. Practically same insight, 80% less time. Thanks to Drs. Gonzalez-Fimbres and Hernandez-Cruz for the collaboration.
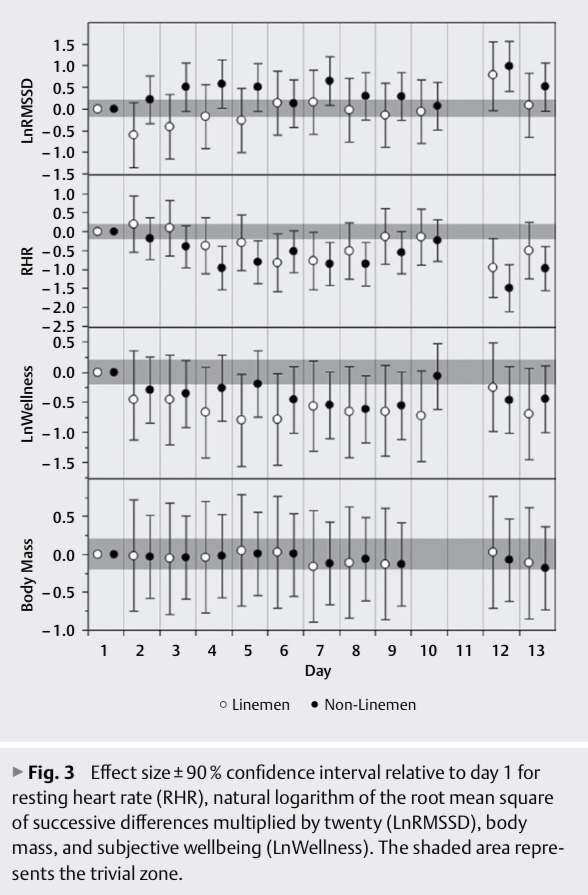
Intensive training periods tend to increase RHR and decrease HRV, reflecting stress and fatigue. However, adaptations to heat exposure (e.g., plasma volume expansion) tend to have the opposite effects. So we wanted to see what happens when players were exposed to both intense training and intense heat stress during preseason camp.
Despite increases in perceived fatigue throughout the 2-week period, RHR and HRV reflected responses consistent with heat acclimation.
HRV initially decreased in linemen, then peaked after a day of rest. Non-linemen faired a little better with smaller decrements in perceived fatigue and more frequent day-to-day improvements in RHR and HRV.
These results indicate that heart rate parameters and perceived fatigue are independent markers of training status, and that desirable cardiovascular adaptations can occur in the presence of soreness and fatigue.
This is especially important for tech companies who try to infer recovery status from HRV alone. As HRV improved throughout camp, an app’s algorithm would report to coaches that players are well-recovered. Given that no player feels well-recovered during preseason camp in the heat, the technology suddenly loses credibility for being wrong and will likely be dismissed.
This is unfortunate because the heart rate parameters are likely reflecting important adaptations that may indicate better tolerance to training in the heat, a reduced exercising heart rate, and improved fitness. Thus, I encourage users to ignore “recovery” scores and interpret the data in appropriate context.
We aimed to characterize cardiac-autonomic responses to a 13-day preseason camp in the heat among an American college football team. Players were categorized as linemen (n=10) and non-linemen (n=18). RHR, natural logarithm of the root-mean square of successive differences multiplied by twenty (LnRMSSD), and subjective wellbeing (LnWellness) were acquired daily. Effect sizes±90% confidence interval showed that for linemen, LnRMSSD decreased (moderate) on day 2 (71.2±10.4) and increased (moderate) on day 12 (87.1±11.2) relative to day 1 (77.9±11.2) while RHR decreased (small–moderate) on days 6, 7, and 12 (67.7±9.3–70.4±5.5 b∙min-1) relative to day 1 (77.1±10.1 b∙min-1). For non-linemen, LnRMSSD increased (small–large) on days 3–5, 7, 12, and 13 (83.4±6.8–87.6±8.5) relative to day 1 (80.0±6.5) while RHR decreased (small–large) on days 3–9, 12, and 13 (62.1±5.2–67.9±8.1 b∙min-1) relative to day 1 (70.8±6.2 b∙min-1). Decrements in LnWellness were observed on days 4–10 and 13 for linemen (moderate) and on days 6–9, 12, and 13 for non-linemen (small–moderate). Despite reductions in LnWellness, cardiac-autonomic parameters demonstrated responses consistent with heat-acclimation, which possibly attenuated fatigue-related decrements.
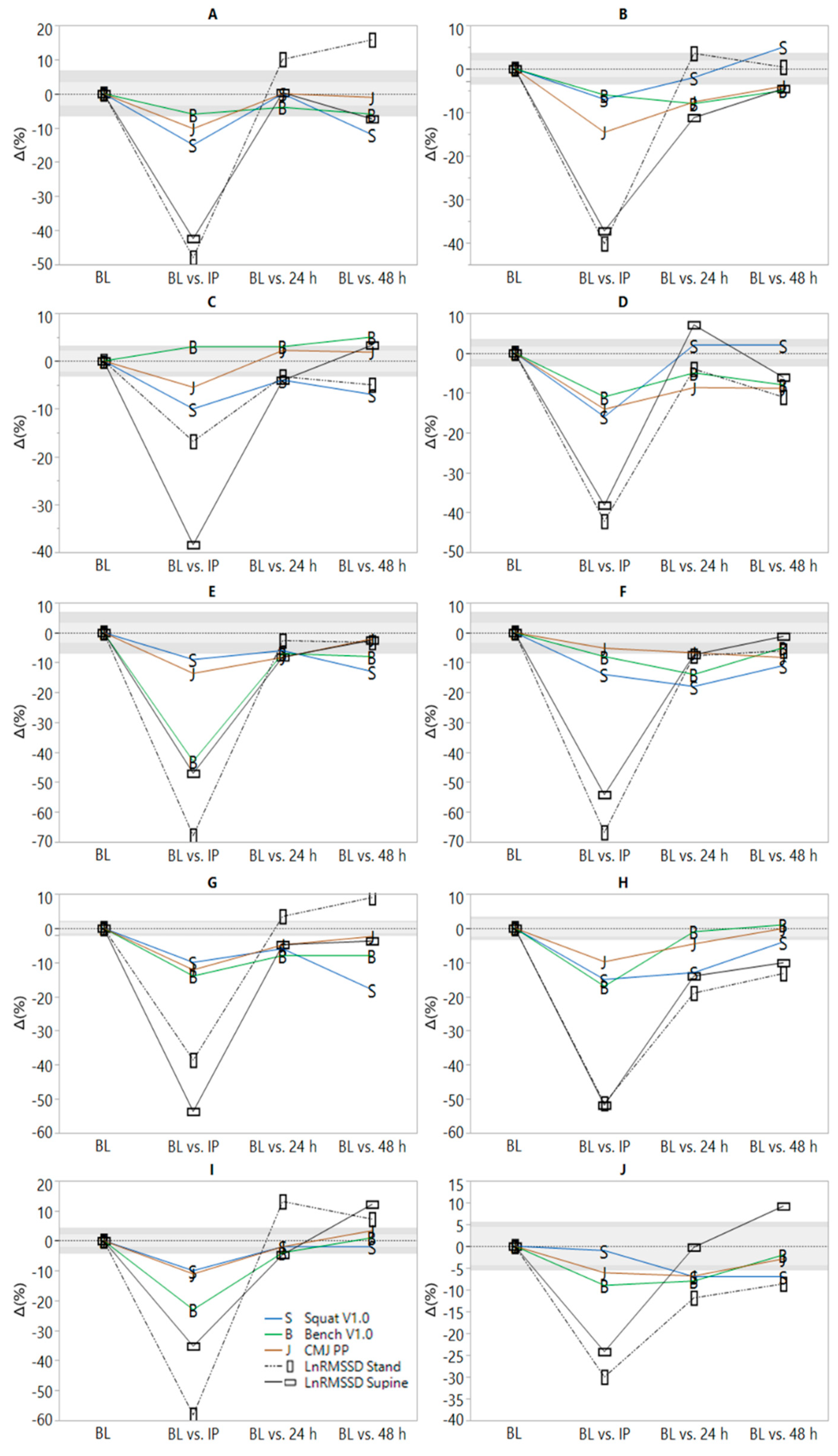
We quantified associations between changes in heart rate variability (HRV), neuromuscular and perceptual recovery following intense resistance training (RT). Adult males (n = 10) with >1 year RT experience performed six sets to failure with 90% of 10 repetition maximum in the squat, bench press, and pull-down. Changes (∆) from pre- to immediately (IP), 24 and 48 h post-RT were calculated for neuromuscular performance markers (counter-movement jump peak power and mean concentric bench press and squat velocity with load corresponding to 1.0 m∙s−1) and perceived recovery and soreness scales. Post-waking natural logarithm of the root-mean square of successive differences (LnRMSSD) in supine and standing positions were recorded pre-RT (5 day baseline), IP and two mornings post-RT. All parameters worsened at IP (p < 0.05). LnRMSSD measures were not different from baseline by 24 h. Neuromuscular markers were not different from pre-RT by 48 h. Perceptual measures remained suppressed at 48 h. No significant associations among ∆ variables were observed (p = 0.052–0.978). These data show varying timeframes of recovery for HRV, neuromuscular and perceptual markers at the group and individual level. Thus, post-RT recovery testing should be specific and the status of one metric should not be used to infer that of another.