After purchasing my HRV device over a year ago I was unsure of whether to take measurements laying down (supine), seated, or standing up. I don’t recall what it was exactly that prompted my decision, but I decided to measure standing. Since day one I’ve recorded my HRV in the exact same position (standing) after waking up for consistency. I often wonder however if this is the best way of measuring HRV for the purpose of monitoring training load, recovery status, etc. I am not an expert on this topic so understand that this article is simply my perspective on the topic based on my experience and research into the matter. Furthermore, I’ve yet to see this discussed in too much depth and therefore decided to investigate the issue myself.
In this discussion I wish to accomplish 3 objectives;
- Briefly discuss the role of the ANS in controlling heart rate at rest and in response to orthostasis (standing up)
- To briefly review some of the research I have read pertaining to this issue
- To present and discuss some data I collected over the last few weeks comparing my morning supine RHR and HRV score vs. my morning standing RHR and HRV score.
Heart Rate Mediated by ANS
Within the wall of the right atrium of the heart is the sino-atrial node (SA node). The SA node randomly initiates impulses that cause the heart to beat. The cardiovascular center of the autonomic nervous system located in the brainstem governs the SA node via parasympathetic and sympathetic innervation. More specifically, the cardiac accelerating center (sympathetic) and cardiac decelerating centers (parasympathetic) of the medulla are responsible for sending sympathetic and parasympathetic impulses to the heart in response to altered blood distribution and pressure requirements (exercise, stress, standing, laying down, etc.)
Sympathetic impulses increase heart rate by exciting the SA node while parasympathetic impulses reduce heart rate by inhibiting it. Thus, with parasympathetic predominance we can expect heart rate to be less frequent and less consistent (more variability between beats) while sympathetic predominance would result in more beats with less variability. *It’s not that simple but for the sake of this article that will suffice*
At times of rest and relaxation, the parasympathetic branch of the ANS will be more dominant whereas during times of stress (exercise, anxiety, etc) the sympathetic branch of the ANS will increase. This is how monitoring our HRV informs us of the balance of the ANS. Though the two branches of the ANS appear to work in a “yin and yang” relationship, both systems are active simultaneously (however to varying degrees). It is possible to have an elevated heart rate and high HRV and vice versa.
During supine, heart rate and blood pressure are lower as the body rests. From supine (a state of high parasympathetic activity and low sympathetic activity) to standing, there is a shift in sympathovagal balance characterised by a withdrawal of parasympathetic activity and a concomitant increase in sympathetic activity (Montano et al. 1994, Mourot et al. 2004). Naturally, the body needs to accommodate for the shift in position forcing the heart to beat harder and faster to pump blood to the brain; a task much less strenuous in the horizontal position.
Some Pertinent Research
Kiviniemi et al. (2007) provides a very thorough explanation of why HRV might be better measured in a standing position as opposed to seated or supine. Essentially, HRV is susceptible to saturation of the parasympathetic nervous system in subjects with low heart rates. Therefore, in athletic populations, changes in parasympathetic activity (as measured by HF Power) may be harder to detect. The author stated “In the present study, endurance training increased HF power measured at standing position but did not change HF power measured at sitting position. This supports our notions that orthostatic stimulus may be more favorable condition than sitting or supine positions to obtain specific information on the status of cardiac autonomic regulation in exercise intervention settings among relatively high fit subjects.”
Uusitalo et al. (1998) saw an increase in sympathetic activity (measured by LF power) measured in overtrained female aerobic athletes in the supine position.
Mourout et al (2004) saw decreased HRV in overtrained athletes compared to not overtrained athletes in the supine position. Similar results were found when HRV was measured after 60 degree tilt. The non-OT group always had higher HRV in the standing position and saw greater reactivity to the postural change.
Uusitalo et al (1999) saw similar results to the work mentioned above by Mourot. Overtrained athletes saw an increase in LF power in the supine position; lower HRV in the standing position; and decreased reactivity to postural change. Additionally, changes in maximal aerobic power were related to decreased HRV in the standing position.
Chen et al (2011) measured HRV in elite weightlifters before during and after an intense workout. HRV was measured in the seated position. The authors found that HRV reflected recovery status as strength levels returned once HRV reached or exceeded baseline in the days following the workout.
Gilder and Ramsbottom (2008) wanted to test whether volume of training load resulted in changes in HRV in response to orthostasis. The authors findings in their words; “Women reporting higher volumes of physical activity had significantly higher levels of parasympathetic HRV than less active women while supine, but also demonstrated a much greater change in parasympathetic HRV in response to standing. It is of interest to note that short-term vagal measures of HRV for HV while standing are similar to those for LV while supine.” *LV=Low Volume HV=High Volume
Grant et al. (2009) found that standing HRV indicators showed significantly more correlations with cardiopulmonary fitness indicators compared to supine measurements. The authors urge practitioners to use caution when attempting to measure fitness via HRV indicating that this is not yet a reliable process.
Hedelin et al. (2001) found that during a 70 degree head up tilt, LF power correlated to measures of strength and aerobic capacity. A greater shift toward LF power in the tilted position correlated to reduced performance. Changes in LF were linearly related to changes in performance suggesting a reflection of adaptation to training.
Hellard et al. (2011) measured HRV in swimmers to model a relationship between HRV and illness. The main results of this study were the following:
“1) In winter, national-level swimmers showed a greater risk of pathology than international-level swimmers. 2) The weeks that preceded the appearance of URTI and pulmonary infection but also MA were characterized by an increase in autonomic parasympathetic activity in supine position. Conversely, in orthostatic position and in winter, the weeks that preceded the appearance of AP were characterized by a drop in parasympathetic activity. 3) During weeks characterized by URTI and pulmonary infection, a shift was noted in the autonomic balance toward sympathetic predominance in supine position and a drop in parasympathetic drive in orthostatic position. And 4) in winter and in orthostatic position, a drop in parasympathetic drive associated with an increase in sympathetic drive was linked to an increased risk of MA.” MA= Muscular Injury, AP=All type pathologies
Huovinen et al. (2009) measured HRV and Testosterone-Cortsiol ratios in army recruits during a week of basic training (class room based). The authors stated; “In the present study, the correlation between the testosterone-to-cortisol ratio and changes in heart rate, SDNN, and high-frequency power expressing an association between circulating ‘‘stress’’ hormones and cardiac vagal activity was apparent in the standing condition only. Thus, based on the results of the present study, measures of heart rate variability should be done not only at rest but also during a controlled sympathetic stimulation (e.g. during an orthostatic challenge).”
Hynynen et al. (2011) looked to compare perceived stress levels with HRV scores during night sleep, supine and after standing. Lower HRV in supine and standing correlated with high stress levels while HRV during sleeping did not.
Iellamo et al. (2004) monitored HRV in elite rowers during overload training and recovery. Measurements were performed in the supine position. HRV decreased with overload and rebounded during a recovery period.
I summarize my thoughts and conclusions on the research at the end of this article.
My Experiment: HRV Supine vs. Standing
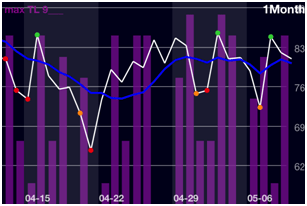
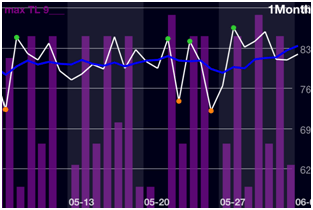
I conducted a small experiment over the last few weeks to see how my HRV responded to supine vs. standing positions. The table below presents the collected data.
|
Date
|
Supine HR/HRV
|
Standing HR/HRV
|
HRV Difference
|
sRPE
|
|
08/10
08/11
08/12
08/13
08/14
08/15
08/16
08/17
08/18
08/19
08/20
08/21
08/22
08/23
08/24
|
52 / 87
51 / 89.5
48.5 / 94.5
49.5 / 88
50 / 88
49 / 90
48 / 92
53 / 92
51 / 101
50 / 85.5
49.5 / 81.5
47 / 90
52 / 90
50 / 83
49.5 / 87
|
56 / 85
65 / 80.5
67 / 84.5
66 / 78.5
67 / 79
61 / 86
71 / 79
69.5 / 80
78 / 73
63 / 79
60.5 / 74.5
58 / 86
75 / 70
65.5 / 84
60.5 / 85.5
|
2
9.5
10
9.5
9
4
13
12
28
6.5
7
4
20
1
1.5
|
8
1
5
7
3
8
3
8
3
0
0
8
3
8
8
|
In interpreting the above data, the majority of the scores appear to give similar data. When reviewing my overall trends (not just these two weeks) usually HR goes up and HRV decreases in response to a high loading day (sRPE 8+). Likewise, HR will decrease and HRV will increase in response to a lower loading day. I’ve found this to be subject to change based on sleep quality and other lifestyle factors that can promote a change in HRV.
I have highlighted three instances that showed conflicting scores. In all three occasions supine HRV is high while standing HRV is low. Each of these conflicting scores occurred on days following a higher intensity workout. Based on my trends and perception of stress I find that the standing scores to be a more accurate reflection of my training load. Generally after an intense workout I’m sore the next morning and fatigued from the workout.
Having said all this, I’m not that smart and can be overlooking something completely obvious. Additionally, these scores (and everyone elses who use a smart phone app HRV device) are subject to the accuracy of the devices (EKG Reciever, Heart Rate strap, etc.) Not to say that they aren’t accurate but it is a potential limitation. Lastly, non-training related stressors are not documented. This is a huge limitation since any form of stress can affect HRV.
Thoughts and Wrap Up (for those still reading)
First and foremost, consistent measurements are more important than position. This is because each of the three positions appear to provide important data regarding training status however, each position provides different data. Therefore, pick a position and stick to it 100% of the time for your values to be meaningful. Switching positions from day to day will provide skewed data.
Endurance athletes and athletes with low resting heart rates are probably better off measuring HRV in a standing position.
Nearly every paper I’ve read on HRV stresses that HRV varies a great deal between individuals. This means that you should not be comparing your data to others. This means that in a team setting, it is important to always compare daily values to baseline (of each individual) for meaningful interpretations. A score of 80 may be high for one individual and low for another.
I like the standing test for the simple reason that it provokes a small stress response. This removes the issues of parasympathetic saturation from the supine position. Seeing how your body responds to standing appears to give you a good idea of how your body can/will handle stress that day. If HRV remains high after standing (given time to stabilize) then you are likely in an adaptive state. If HRV is low after standing (given time to stabilize) you are likely less adaptive (currently under higher stress).
HRV test length may influence positional preference. Measuring HRV for 3+ minutes may be more comfortable in a supine or seated position. My device (iThlete) is a 1 minute test and therefore I don’t find the standing position to be a nuisance. However, I did prefer the supine measurements simply because I only needed to focus on breathing and nothing else.
It may be optimal to measure HRV in both supine and standing positions for more complete data. I’ve seen several papers that measure supine-standing-supine HRV (orthoclinostatic measurements). Though this is less convenient and less practical, it may provide more accurate information.
Lastly and most importantly, the research is conflicting and more needs to be done. Formulate your own opinion based on the research and apply it to yourself. Consider experimenting by recording data in various positions, compare it to perceived stress (training, mental, chemical, etc) and determine what you like best. If you do perform this experiment be sure to only save the data on the app for your preferred testing position to keep meaningful trends and daily color indications.
References:
Chen, J. et al. (2011) Parasympathetic nervous activity mirrors recovery status in weightlifting performance after training. Journal of Strength and Conditioning Research, 25(6): 1546-1552
Gilder, M., & Ramsbottom, R. (2008) Change in heart rate variability following orthostasis relates to volume of exercise in healthy women. Autonomic Neuroscience: Basic & Clinical, 143(1-2): 73-76
Grant, C. et al. (2009) Relationship between exercise capacity and heart rate variability: supine and in response to an orthostatic stressor. Autonomic Neuroscience: Basic & Clinical, 151(2): 186-188
Hedelin, R., et al. (2001) Heart Rate Variability in athletes: relationship with central and peripheral performance. Medicine & Science in Sports & Exercise, 33(8), 1394-1398.
Hellard, P., et al. (2011) Modeling the Association between HR Variability and Illness in Elite Swimmers. Medicine & Science in Sports & Exercise, 43(6): 1063-1070
Huovinen, J. et al. (2009) Relationship between heart rate variability and the serum testosterone-to-cortisol ratio during military service. European Journal of Sports Science,9(5): 277-284
Hynynen, E. et al. (2011) The incidence of stress symptoms and heart rate variability during sleep and orthostatic test. European Journal of Applied Physiology, 111(5): 733-41
Iellamo, F. et al. (2004) T-wave and heart rate variability changes to assess training in world class athletes. Medicine & Science in Sports and Exercise, 36(8): 1342-1346.
Montano, N. et al. (1994) Power spectrum analysis of heart rate variability to assess the changes in sympathovagal balance during graded orthostatic tilt. Circulation, 90: 1826-1831 Free Full Text
Mourot, L. et al (2004) Decrease in heart rate variability with overtraining: assessment by the Poincare plot analysis. Clinical Physiology & Functional Imaging, 24(1):10-18.
Uusitalo et al. (1998) Endurance training, overtraining and baroreflex sensitivity in female athletes. Clinical Physiology, 18(6): 510-20
Uusitalo et al. (1999) Heart rate and blood pressure variability during heavy training and overtraining in the female athlete. International Journal of Sports Medicine, 20: 45-53